The discussion from episode 146 between 56’ and 1:00’ confused the heck out of me. It was the exchange between @trevor and Dr. Coyle regarding training for maximum stroke volume. Trevor brought up an article that attempted to show that it was more effective to train such that there is very low heart rate instability (drift) using low intensity intervals. In the discussion it was unclear what effect was actually observed in the study.
In his reply Dr. Coyle stated that he believes that the best training to increase stroke volume is the 5 minute all-out VO2 max interval (an interval that, per previous podcasts, I believed was to be avoided at all costs).
What was confusing about this exchange is that you guys seemed to conflate stroke volume with total oxygen flux (essentially a percentage of VO2max) as the stimulus and/or training adaptation being sought. Logically, it would seem that the stimulus would be related to oxygen flux: if the muscle is being asked to do more work than it can with the available oxygen, it makes sense that it would start sending adaptation signals. But is increased stroke volume the adaptation that happens? And how? I had understood that increased plasma volume is an adaptation that happens. This thins the blood and allows a higher velocity flow (but doesn’t that reduce the hemoglobin concentration/hematocrit count?). Regardless, I don’t see how stroke volume would change unless the heart itself is growing.
Anyway, I’m confused. Can you please clarify a bit?
Last thing: I was also wondering if you guys had thought to get into it on the all-out “VO2 max” effort. Seems to me that there should be a balance between providing the absolute maximum stimulus by maximizing oxygen flux (and the potential negative stress response of that) vs. extending the time period over which the large oxygen flux is demanded.
Wouldn’t oxygen flux and stroke volume be two different adaptations from high intensity exercise? The former occurring peripherally at the working muscle, the latter occurring centrally at the heart? Related to the same underlying metabolic stress/strain, but not from the same stimuli?
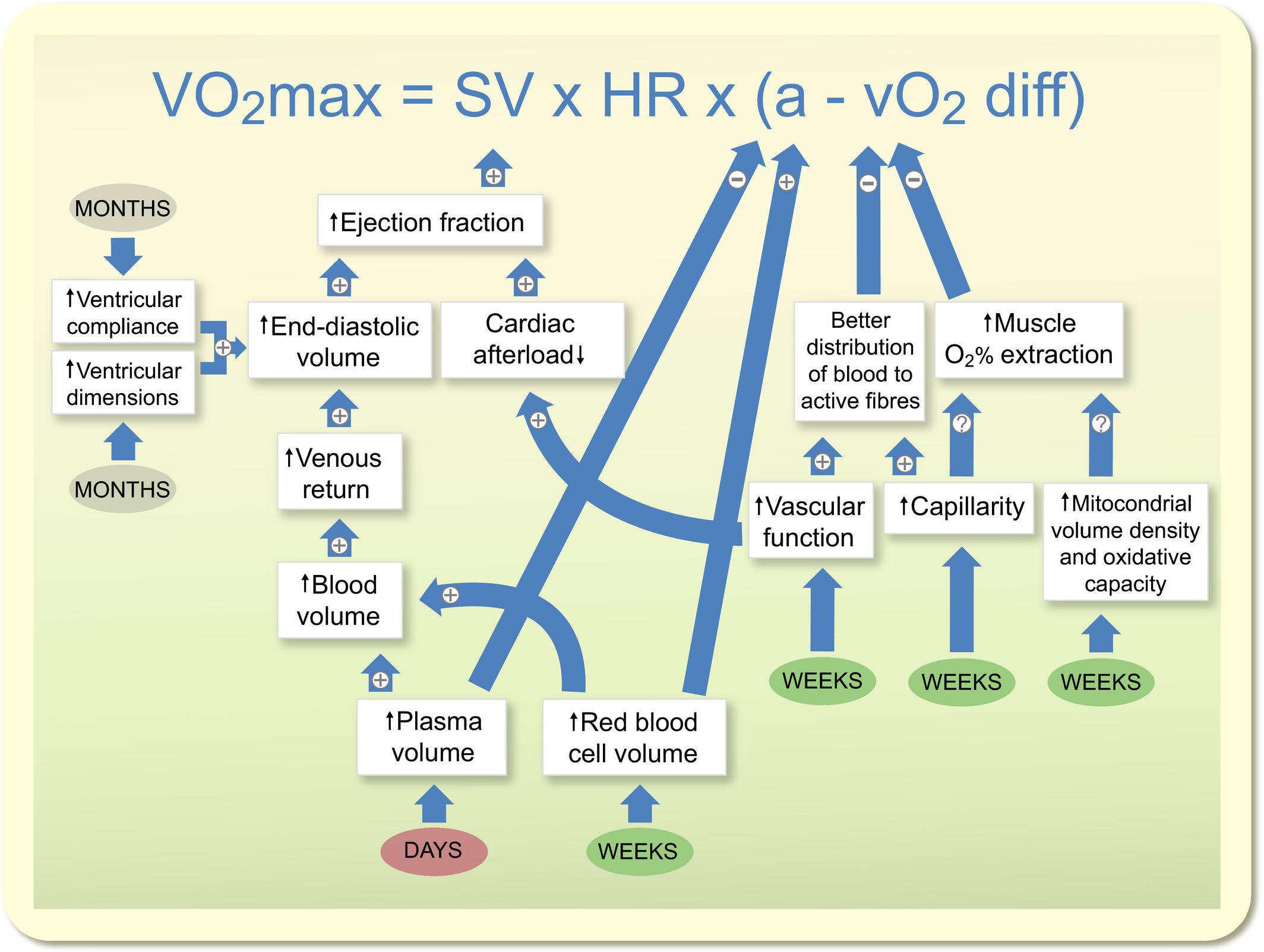
Enhanced stroke volume occurs as a short-term functional adaptation, as the ability of the heart to stretch and pump greater blood volume on each beat. This is related to increases in plasma volume. Increased blood volume ⇒ greater venous return ⇒ greater filling of the heart ventricles ⇒ greater stroke volume. Long-term this does cause morphological/structural change to the heart to further increase stroke volume.
This might be helpful to understand some of the adaptations
Your last point is a good one too IMO. Yes, a maximal intensity interval might be optimized for acute stimuli from a single interval workout, but is that sustainable over longer term? Is repeating all-out interval workouts optimal as part of a longer training block?
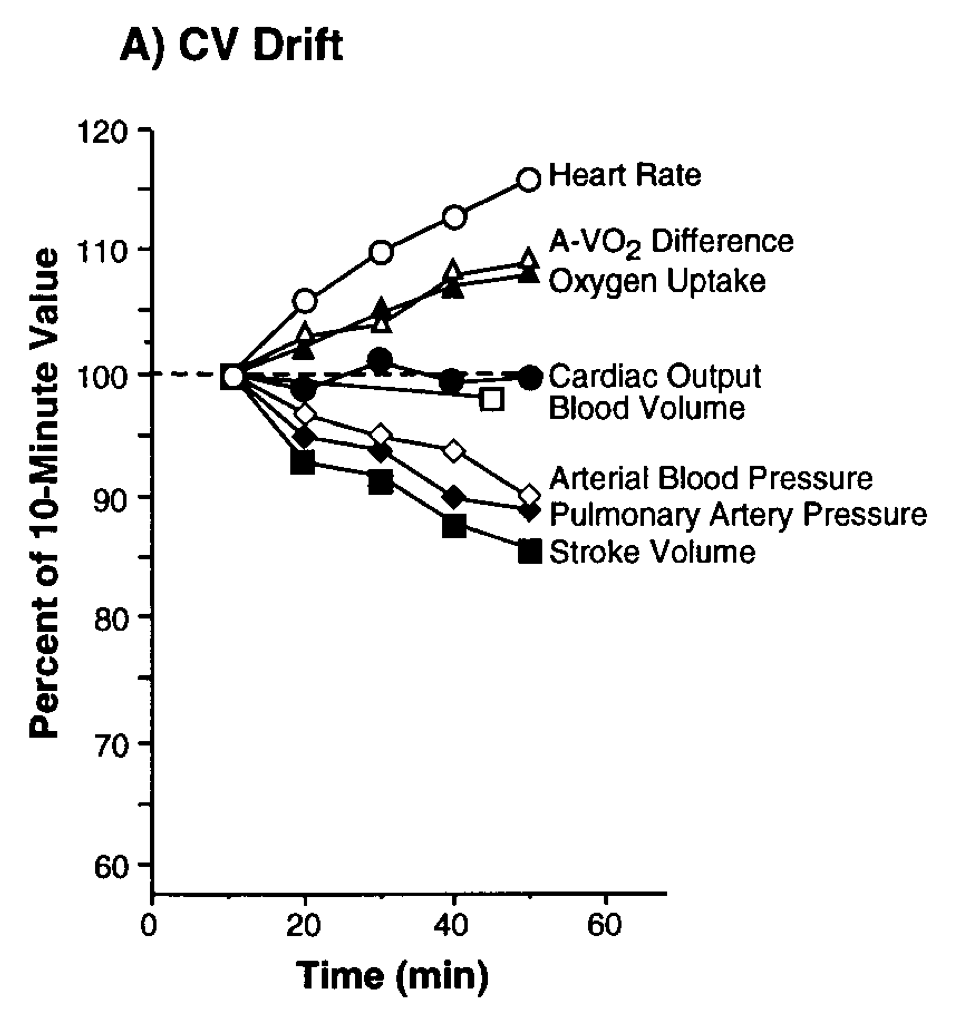
Hi @SteveHerman, great questions! I’m sure Trevor will jump in when he gets the chance, but I’ll start with some thoughts to your questions. I did listen to the episode and can see where some of that confusion might have come up. My take was that the low intensity study seemed to show that with consistent riding there was cardiovascular drift occurring, which limited the time to 1.5 minutes at SVmax via the continuous rise in HR and decline in SV. So switching to 3x intervals of ride time, it would seem that they were able to achieve ~8 minutes at SVmax by building in those recovery periods before SV begins to decline and CV drift really sets in.
There is support for high intensity training to improve VO2 max, and SV is one of those central adaptations. You’re right about the increased plasma volume as well. The increased PV is a hallmark of elite level athletes, and one of the benefits is increasing the heat offload to the periphery.
The mechanisms for SV increases are complex, maybe a bit much for one forum post, but to try and keep it somewhat brief we are looking at structural and functional changes to the left ventricle. Your comment about not seeing how SV would change unless the heart is growing is excellent. There are changes that take place that improve contractility and left ventricular function through training, and these changes are part of the mechanism for improvement. Regarding the heart growing, there was an interesting paper on older men and women where it showed that the women experienced basically no changes in the heart structure, and most of their improvements in VO2 max were due to the a-vO2 difference.
I think to your last point on the all-out VO2 max effort is great. I do agree with you on the balance. It’s not a requirement to go balls out on VO2 max efforts to get the adaptive responses. Can you? Sure. When I was running and racing a lot in my 20s I would do 1-2 workouts of 5x 5-6 minutes all-out, but I could recover from it. Now, I’m not hitting those in the same way due to the potential negative stress and added recovery, as you suggested. If you look at a lot of the health research you can get benefits in VO2 max from moderate intensity continuous training and high intensity training at 85-95% maximum. There will of course be higher and lower responders within these groups and it’s not a one-size-fits-all with the training approach, but my point is that you can get there a number of ways, and your suggestion of finding a balance is spot on.
@SpareCycles, great point, and thank you for posting that informative graphic!
I’ve seen some of those shorter interventions, 2-6 weeks roughly, supporting the peripheral adaptations (a-vO2 diff), but it does seem to take longer before those central adaptations (SV) begin to take hold. There was a study from 1997 that looked at quite a short period of time (10 days of exercise) and it showed improvements, but a-vO2 diff was unchanged, as expected based on your reference above. So it’s interesting to look at the time course of these adaptations and think about our training blocks.